How do your clients or even your own MIP compare to a Super Rugby player?
- 17 October 2019
As we move into summer in the southern hemisphere we are all able to get outside and push into the sports we enjoy.
In spring and summer many people experience breathing dysfunction with high VO2 max sports such as swimming, rowing, cycling and running as respiratory demand is very high.
Breathing Dysfunction in Sports
Common causes of shortness of breath in exercise include: asthma, exercised induced asthma, vocal chord dysfunction (VCD or EILO), sports related anxiety, hyperventilation or breathing dysfunction, cardiovascular disease, lung disease, anaemia or obesity. With a long list like this it is difficult to know where to start!
Blood tests and simple lung function testing (spirometry) can help rule in our out anaemia or asthma, as can ECG and cardiology referral for heart problems. VCD is tricky to diagnose and is easily mistaken for asthma but usually the wheeze is felt on inhaling rather than exhaling. What about dysfunctional breathing?
How do you compare to elite sports people?
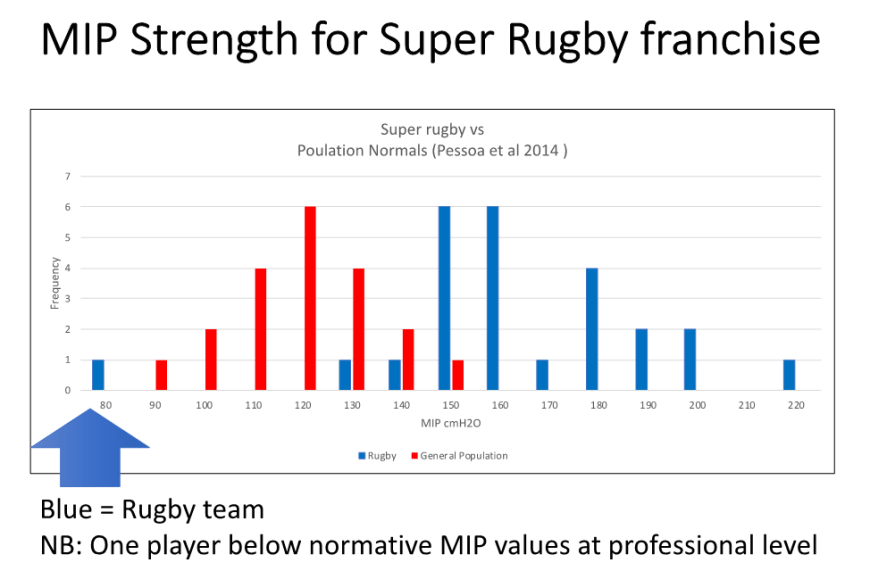
This year we have had the privilege of working with a number of elite athletes, and have tested their Maximal Inspiratory Pressure (MIP). Check the stats below to see where your client or yourself sit compared to other athletes!
There is no known prevalence data of dysfunctional breathing. Measurement of respiratory strength has been recently discussed in an excellent review study, and it is great to see that BradCliff practitioners are aware and some already practicing to an international standard in this area using MIP and diaphragm thickness in testing athletes.
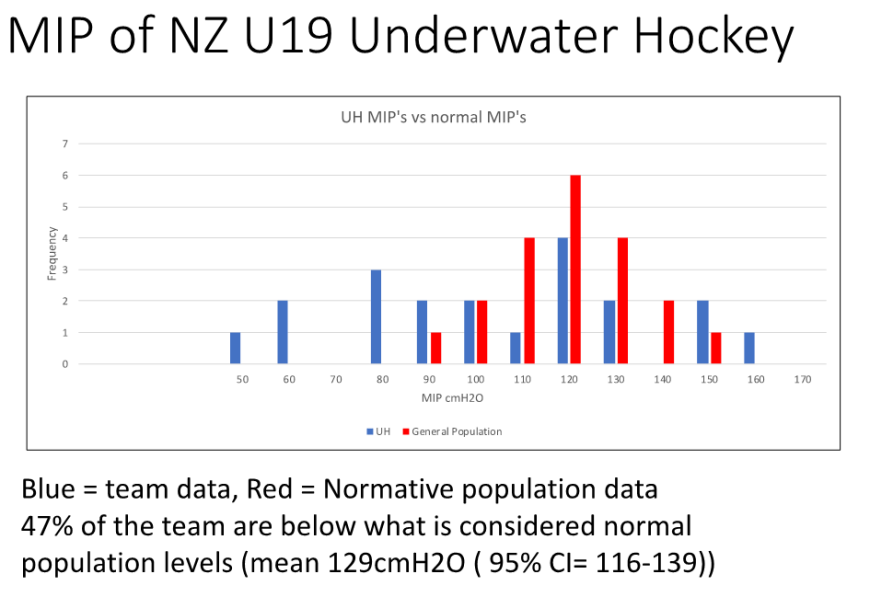
In one sub-elite National team (Under 19 age group), 47% of the team had inspiratory muscle strength that was below the normative levels published for this age group. Another group of professional rugby players (NZ Super Rugby Franchise) had markedly different results with only one player with low inspiratory strength, and almost 90% of the players exceeding normal levels.
Weakness versus Symptoms
Weakness of respiratory muscles comprises one component of breathing dysfunction (biomechanical, biochemical and psychophysiological comprising the others). The ideal situation is that the diaphragm and lower 6 ribs produce an outwards (bucket handle) motion. Under heavy loading and repetitive mouth breathing, this can change to being more vertical. If this non-optimal pattern is repetitively loaded in sport, the diaphragm may eventually weaken and the smaller accessory muscles strengthen which can create a cycle of shortness of breath, chest pain and neck, rib or back pain..
“People don’t realise how drastically a bad breathing technique can affect them, but by learning how to breathe properly the effects can be literally life changing.”